
Surgery & Anesthesia
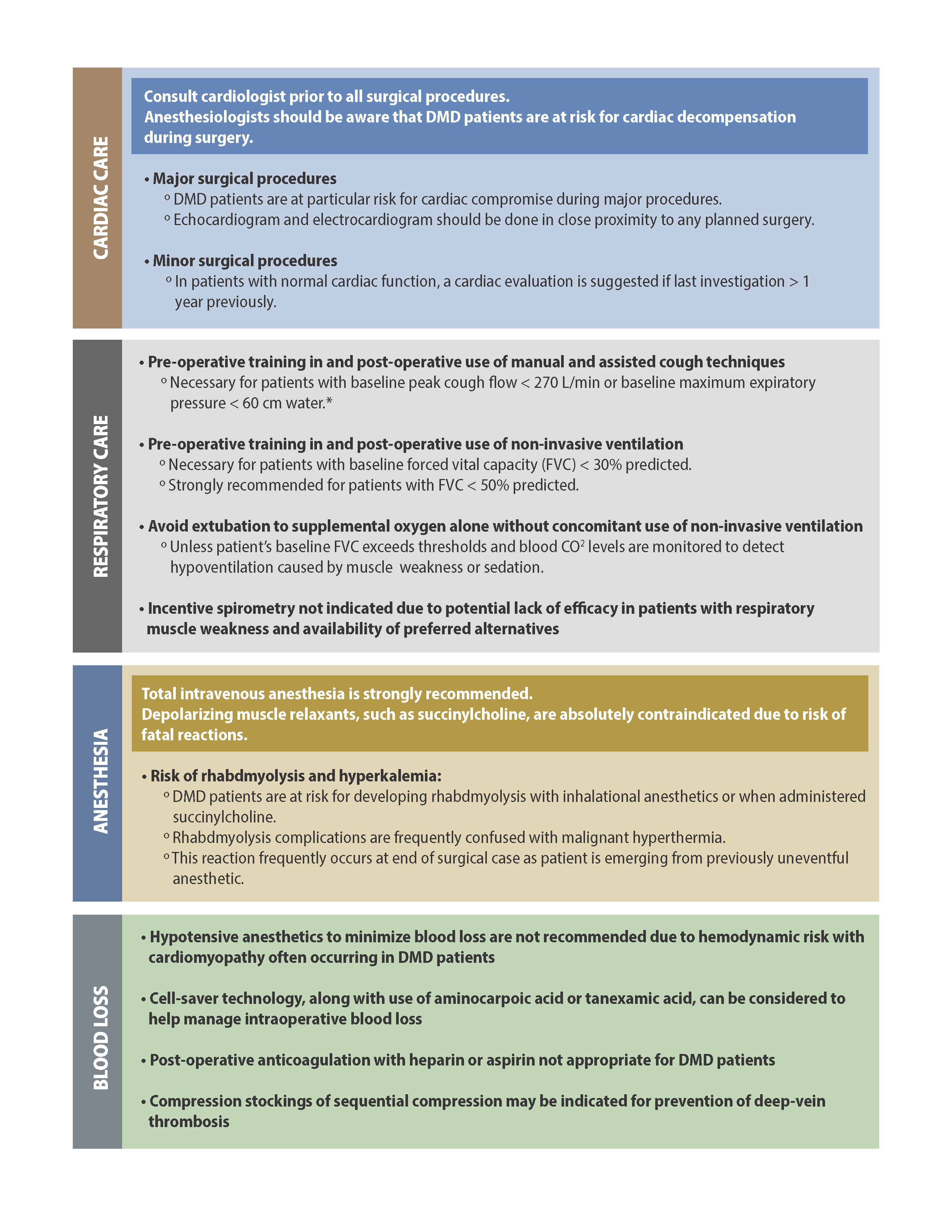
When a patient with Duchenne or Becker muscular dystrophy has general anesthesia, a number of issues should be considered, including cardiac and pulmonary function, anesthesia, and the potential for blood loss.
*Note precautions extend to both Duchenne and Becker, but for simplicity we primarily refer to Duchenne.
Considerations for Surgery & Anesthesia
If you require surgery or a medical procedure, go to a medical center with expertise in the anesthetic management of people living with Duchenne and Becker if possible. Your anesthesiologist should be aware that you have Duchenne or Becker. It is important to discuss the anesthesia plan with your anesthesiologist before any surgery or procedure that involves anesthesia.
*If your child is taking steroids, you should share the PJ Nicholoff Steroid Protocol with your medical team prior to surgery. Steroid stress doses are needed during/after surgery to prevent life threatening adrenal crisis.
Additionally, your neuromuscular team should always be made aware if you are undergoing surgery or a medical procedure. Additionally, you should have evaluations by your cardiologist and pulmonologist before undergoing any type of surgery or medical procedure. Any cardiac and/or respiratory abnormalities should be identified and optimally treated before any surgery or procedure involving anesthesia.
These recommendations have been reviewed and approved by the Professional Advisory Council of the Malignant Hyperthermia Association of the U.S. (MHAUS). Discuss risks and benefits of planned anesthetic medications (agents) with your anesthesiologist.
Anesthesia agents requiring caution in Duchenne
People with Duchenne should NOT receive succinylcholine.
The drug succinylcholine (suxamethonium) is a depolarizing muscle relaxant. It is sometimes used in emergencies to relieve breathing difficulties in anesthetized patients. However, when succinylcholine is administered to patients with any kind of ongoing muscle atrophy, no matter the underlying cause, succinylcholine can cause severe, life-threatening (and sometimes fatal) increases in blood potassium.
Instead of succinylcholine there are other commonly available muscle relaxants (e.g., any non-depolarizing neuromuscular blocker) that can be used in emergency situations if necessary (see the “Safe” list section below). It is possible, however, that there exists a rare situation (such as life-threatening airway obstruction that requires immediate treatment) where an anesthesiologist may be justified in administering succinylcholine to a patient with Duchenne whose life is in imminent danger.
Avoid inhaled anesthetic agents if possible.
Commonly used inhaled anesthetic agents include Desflurane, Enflurane, Halothane, Isoflurane, and Sevoflurane.
People with Duchenne are at risk of developing rhabdomyolysis (the breakdown of skeletal muscle tissue that may cause the release of myoglobin that can damage the kidneys) and hyperkalemia (the release of too much potassium into the bloodstream), which can result in life-threatening heart rhythms.
There are known cases of serious (and sometimes fatal) muscle breakdown (rhabdomyolysis) in Duchenne patients when exposed to inhalation anesthetic gases even when succinylcholine was avoided. Therefore, we recommend that when possible, inhalational anesthetic gases should be avoided or used sparingly in people with Duchenne. However, there are certain circumstances when the benefit/risk ratio favors the use of these inhaled agents. The administration of inhaled anesthetic agents may be suggested for the following reasons:
- Prior to IV catheter insertion
The only other type of anesthetic agents are given intravenously (through an IV catheter). Inserting IV catheter can be painful, and people with Duchenne may require multiple sticks due to difficulty finding veins in people with decreased muscle mass. Giving inhaled anesthetic before the nurse attempts an IV stick can reduce the pain and make it easier to obtain IV access. - Propofol administration
The drug Propofol is a commonly used IV anesthetic agent for procedures. However, it can be very painful when it starts infusing through an IV. Sometimes inhaled anesthetic agents will be given before Propofol is started to avoid the pain of the infusion. - IV anesthesia is not available
There may be rare situations where IV anesthesia is not available, or is considered an inferior anesthetic choice based on the patient’s specific clinical situation.
Am I at risk for “malignant hyperthermia?”
Among anesthesiologists, it is established knowledge that patients with Duchenne muscular dystrophy may develop unique complications when undergoing medical or surgical procedures that require certain anesthetic agents (discussed above). The complications including rhabdomyolysis and hyperkalemia are nearly indistinguishable from those seen when a patient develops a rare anesthetic-related complication called malignant hyperthermia (MH).
Although clinically similar in appearance to the complications that may occur in Duchenne patients, they are actually two separate entities. MH is typically an inherited genetic condition that has nothing to do with the dystrophin gene.
Because of the similar symptoms of these two complications, there was a time when many clinicians believed that the anesthesia complications in Duchenne patients were, in fact, MH. However, after studying this over the years, we now know that this isn’t true. MH occurs in patients who have inherited MH-causing mutations, which people with Duchenne are not at a higher risk for than the general population.
Duchenne patients are not at an increased risk of developing MH, but may continue to be at increased risk of rhabdomyolysis when administered inhaled anesthetic gases. These guidelines have been reviewed and approved by the Professional Advisory Council of the Malignant Hyperthermia Association of the U.S. (MHAUS).
Safe anesthesia
All intravenous (IV) anesthetic agents are considered to be safe to give to people with Duchenne with close monitoring.
- Barbiturates/Intravenous Anesthetics
Diazepam (valium), Etomidate (Amidate), Ketamine (Ketalar), Methohexital (Brevital), Midazolam (Versed), Propofol (Diprivan), Thiopental (Pentothal) - Inhaled Non-Volatile General Anesthetic
Nitrous Oxide (“laughing gas”) - Local Anesthetics
Amethocaine, Articaine, Bupivicaine, Etidocaine, Lidocaine (Xylocaine), Levobupivacaine, Mepivicaine (Carbocaine), Procaine (Novocain), Prilocaine (Citanest), Ropivacaine, Benzocaine (caution re: methemoglobinemia risk), Ropivacaine - Narcotics (opiods)
Alfentanil (Alfenta), Codeine (Methyl Morphine), Fentanyl (Sublimaze), Hydromorphone (Dilaudid), Meperidine (Demerol), Methadone, Morphine, Naloxone, Oxycodone, Remifentanil, Sufentanil (Sufenta) - Muscle Relaxants
Arduan (Pipecuronium), Curare (The active ingredient is d-Tubocurarine), Metocurine, Mivacron (Mivacurium), Neuromax (Doxacurium), Nimbex (Cisatracurium), Norcuron (Vecuronium), Pavulon (Pancuronium), Tracrium (Atracurium), Zemuron (Rocuronium) - Anticonvulsants
Gabapentin (Neurontin), Topiramate (Topamax) - Anxiety Relieving Medications
Ativan (Lorazepam), Centrax, Dalmane (Flurazepam), Halcion (Triazolam), Klonopin, Librax, Librium (Chlordiazepoxide), Midazolam (Versed), Paxipam (Halazepam), Restoril (Temazepam), Serax (Oxazepam), Tranxene (Clorazepate), Valium (Diazepam)
See a complete list of Safe and Unsafe Anesthetics.
Supplemental Oxygen
Because people with with Duchenne have weak respiratory muscles, their diaphragms do not move up and down well and their intercostal muscles (the muscles that move the chest walls) do not expand the ribs well. This causes shallow breathing, but people with Duchenne compensate for this over time, and can provide the body with adequate oxygen supply and adequate removal of carbon dioxide. During surgery or procedures, certain anesthetics may lead to increasingly shallow breathing. Too shallow of breathing (hypoventilation) may lead to low oxygen levels and high carbon dioxide levels.
Your anesthesiologist may decide you will need supplemental oxygen during your procedure, but they must use caution. When extra or supplemental oxygen is given, this delicate balance is disturbed. The respiratory center may get the false impression that the body has enough oxygen and no longer needs to breathe. Without breathing, carbon dioxide can build to dangerous levels (called hypercapnia). If oxygen is required during surgery or medical procedures, the anesthesiologist must use caution and monitor you closely. They may also use non-invasive ventilation (i.e. BiPAP machine) during the procedure to ensure you are breathing adequately.
Endotracheal Tubes
During surgery, it is sometimes necessary to support your breathing due to anesthesia or muscle relaxants given during the procedure. Intubation involves putting a breathing tube (also known as an endotracheal tube) into your airway. This breathing tube is then connected to a breathing machine (respirator or ventilator). This machine will then either assist with your breathing or actually breath for you, depending on your pulmonary function, the length of the surgery, or the type of surgery. Intubation is usually done after you have received anesthesia and are asleep. The anesthesiologist will monitor you closely and control the ventilator. The tube will usually remain in and connected to the machine until the surgery is completed.
After the surgery, the breathing tube must be removed. The process of removing the breathing tube is called extubation. Because breathing tubes were sometimes, in the past, left in place too long or were removed incorrectly, a protocol for extubation was developed by Drs. Mary Schroth and John Bach. When you meet with your anesthesiologist before surgery, be sure you discuss the intubation/extubation and show them the protocol.
Dental Procedures
Dentistry generally can, and should, be performed with the minimal amount of anesthesia possible while providing the patient maximal physical and emotional comfort. Local anesthetics, nitrous oxide, and an oxygen “wash out” are safe for most patients with Duchenne, especially patients who are ambulatory with normal pulmonary function (normal breathing).
Patients with Duchenne who have pulmonary dysfunction (abnormal breathing) should consider receiving dental care requiring general anesthesia in a hospital or surgery center staffed with an anesthesiologist, and equipped to monitor intra-operative respiratory functioning and to manage potential respiratory and cardiac emergencies. Visit this page for more information concerning dental procedures.



