Recommended Care
The information on this page represents the recommended standard of care for Duchenne muscular dystrophy. Most of the care recommendations also apply to Becker muscular dystrophy, but at older ages. Most, but not all, people with Duchenne are males—but the care recommendations apply to both males and females with Duchenne.
If you don’t understand any of the medical terms and concepts, ask your healthcare providers. Take notes and ask questions during your clinical visits.
When to start taking steroids
Steroids should be discussed near the time of diagnosis with your neuromuscular specialist. Steroids should be started before your child reaches the “plateau phase” and loses any significant strength – this is generally around age 4-5 years. In Duchenne, the plateau phase is when your child:
- Has learned all of their motor skills (crawling, walking, climbing stairs)
- Is having minimal trouble walking
- Can rise from the floor with little to no effort
- Can climb stairs with little to no effort
In other words, when your child is still able to physically do things in a way that is similar to their peers, it is the best time to start steroids.
Understanding steroid dosing
- The recommended starting dose of daily prednisone is 0.75 mg/kg/day. The recommended starting dose of daily deflazacort is 0.9 mg/kg/day. The recommended starting dose of daily Agamree (vamorolone) is 2mg-6mg/kg/day.
- Your neuromuscular specialist (NMS) may increase or decrease the dose based on growth, weight, and other side effects experienced.
- Steroids have been prescribed and taken in many doses and using many different schedules.
- In the US, dosing is either daily or high dose weekends. In some countries, other dosing schedules (i.e, 10 days on, 10 days off, etc.) have been used.
- Vamorolone should not be used for intermittent or weekend-only treatment.
- The impact that steroids have on the body depends on the dose of the steroid and how often the steroids are taken.
- People who are taking intermittent doses (i.e., not daily) may have fewer or less severe side effects.
Is there a maximal dosing of steroids in Duchenne?
- Due to the effects of daily steroids on the body, as well as the risk of side effects with higher doses, daily steroids are not prescribed in doses higher than around 36 mg/day of prednisone or 40 mg/day of deflazacort, or 300mg/day of vamorolone.
- While the FOR-DMD study is looking at dosing, there currently is no information around the maximal dosing of steroids in Duchenne.
- Generally doses of twice weekly steroids can go up to 250 mg/day of prednisone (or 300 mg/day of deflazacort, which is comparable to the prednisone weekend dose, but has not been studied) given on weekends.
What else do I need to know about steroid dosing?
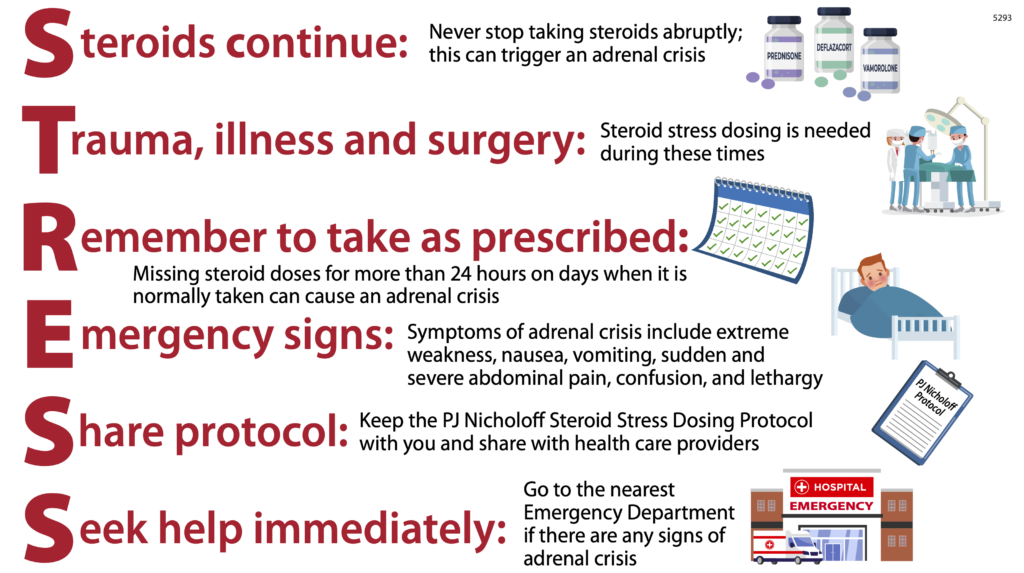
Adrenal suppression, or adrenal crisis, is a potentially life-threatening complication of steroid use. It is important to remember the following information:
- Do not stop taking steroids suddenly.
- Do not miss daily steroid doses for more than 24 hours (i.e. accidentally missing a dose, vomiting more than 24 hours, hospitalization without continuation of medication, etc.).
- Know when “stress doses” should be given (severe illness, surgery, or trauma).
*Vamorolone cannot be used for stress dosing and it is unknown if deflazacort is appropriate for stress dosing. Refer to the PJ Nicholoff Steroid Protocol (download) for stress dosing guidelines.
Maintenance doses and stress dosing considerations for glucocorticoids in Duchenne muscular dystrophy and other dystrophinopathies
| Gluccocorticoid | Used for DBMD Treatment | Maintenance dose1
| Half-life (hours)2 | Gluccocortiod receptor activity | Mineralocorticoid receptor activity | Appropriate for stress coverage3 |
| Hydrocortisone | NO
| 8-10 mg/m2/day | 3 | Agonist | Agonist | YES |
| Prednisone | YES | 2-3 mg/m2/day | 6.2 | Agonist | Agonist | YES |
| Prednisolone | YES | 2-3 mg/m2/day | 6.2 | Agonist | Agonist | YES |
| Deflazacort | YES | 2.6 mg/m2/day4 | 1.1 to 1.9 | Agonist | Weak agonist | UNKNOWN5 |
| Vamorolone | YES | Unknown | 2 | Agonist | Antagonist | NO |
1 Expressed as mg/m2 of body surface area (BSA)/day. There are multiple equations for calculation of BSA, the equation used in the local electronic health record or practice is encouraged. BSA can also be estimated from weight alone: (weight (kg) × 4) + 7/(weight (kg) + 90)
2 Clinically a drug is considered to be eliminated from the body after 4-5 half-lives
3 See Tables 5 and 6 for stress dosing details
4 Estimates based on historically accepted conversion factors and should be considered a guide only. Deflazacort is not recommended for maintenance replacement.
5 Insufficient data to inform stress dose or frequency. Use with caution
Abbreviations: DBMD, Duchenne and Becker Muscular Dystrophy and other dystrophinopathy
More information on these important topics can be found here.


 FAQ: Choosing a Steroid Drug, Dose, and Regimen
FAQ: Choosing a Steroid Drug, Dose, and Regimen


