
What does it mean to have germline mosaicism?
Germline mosaicism means that a person has a genetic variant that is present in some of their egg or sperm cells, but not all of them. Most carriers for dystrophinopathy have the DMD gene variant in every cell of their body. However, there are some women who will have a DMD gene variant in multiple egg cells, but not in other cells of their body. These women are said to have germline mosaicism.

Germline mosaicism was first recognized in dystrophinopathy when it became apparent that some women with negative genetic testing had more than one child with Duchenne. Carrier testing typically uses blood or saliva, which means it cannot identify when a person has the DMD gene variant only in their egg cells.
Germline mosaicism is not believed to be very common, although it is almost impossible to determine how many women have germline mosaicism. The majority of carriers of a DMD gene variant carry the variant in every cell of their body.
There are not likely to be any health concerns for women with germline mosaicism. The cells in the rest of their bodies have two working copies of the gene, so it is possible that females with germline mosaicism have no increased chance for skeletal muscle symptoms or heart changes, though studies have not been done to confirm this.
How is germline mosaicism found?
Women with germline mosaicism will not be found to be carriers via genetic carrier testing, because carrier testing is done on blood or saliva cells. Women with germline mosaicism have genetic variants in their egg cells, which will not show up on the blood or saliva test.
Because lab testing cannot identify germline mosaicism, healthcare providers are left to assume that germline mosaicism explains most cases where females have no DMD variant found on carrier testing but have more than one affected child.
All women who have an affected child and no DMD variant found on carrier testing have a small chance to have germline mosaicism. It is not known exactly how often this happens, though a recent study reviewing the literature about germline mosaicism in dystrophinopathy found evidence for germline mosaicism in 8.1% of de novo families (families in which it seems an affected child is the first one with a variant). This report also found that the chance for a woman with negative carrier testing and one affected son to have another affected child ranged from 4.3% to 11%, with an average of 5.8%.
HOW IS DUCHENNE PASSED THROUGH WOMEN WITH GERMLINE MOSAICISM?
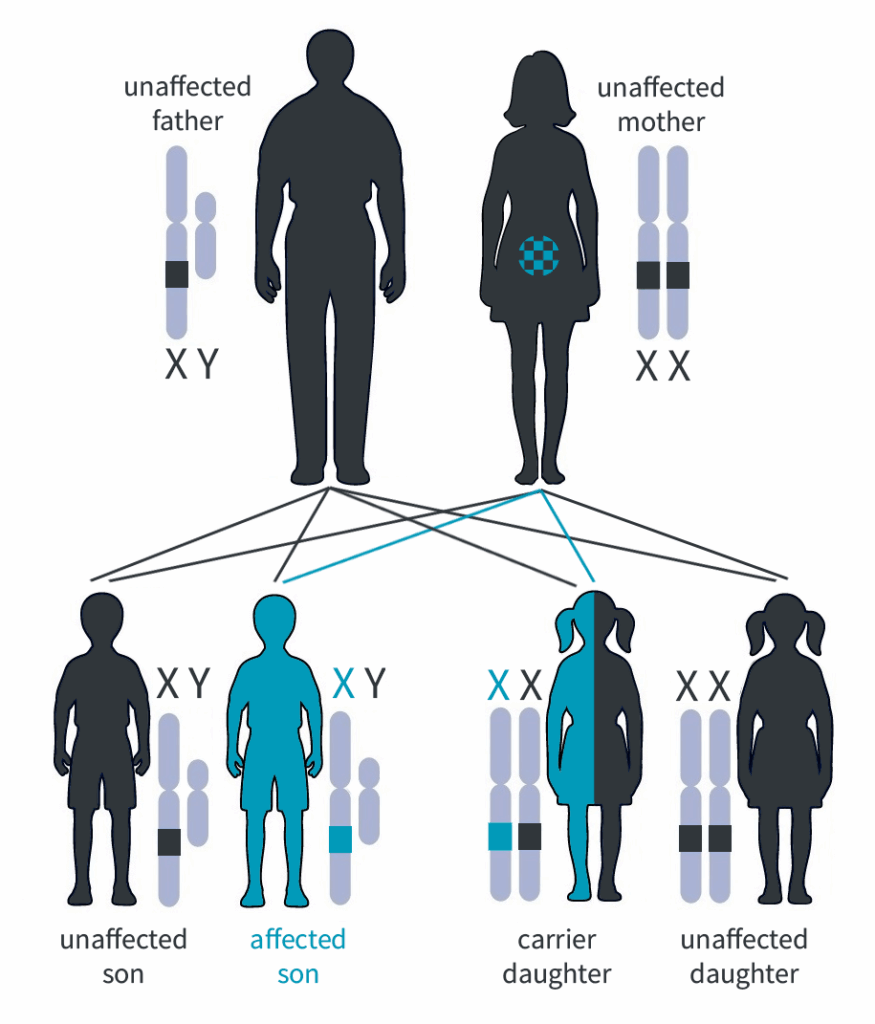 Females with germline mosaicism have an increased chance to have children born with dystrophinopathy, but the exact chance is impossible to know. Females with germline mosaicism can pass to their children, either:
Females with germline mosaicism have an increased chance to have children born with dystrophinopathy, but the exact chance is impossible to know. Females with germline mosaicism can pass to their children, either:
- An egg with a working copy of the dystrophin gene, resulting in no increased chance for dystrophinopathy, or
- An egg with the copy of the dystrophin gene with a variant, resulting in an affected son or a carrier daughter (who could have no symptoms or could be a manifesting carrier).
The chance to have a child with dystrophinopathy depends on the amount of eggs with the working copy of the dystrophin gene versus the amount of eggs with a dystrophin gene variant. The chance could be higher or lower than 50%. Unfortunately, it is not possible to tell how many egg cells have the dystrophin gene variant.
For this reason, all women who have one affected child should be offered prenatal testing in future pregnancies, regardless of whether their carrier testing was positive or negative. Learn more about prenatal testing and other reproductive options.



